Perimenopause Skin Symptoms Explained
If your face feels tight in some areas and greasy in others, perimenopause may already be changing your hormones — even if you haven’t noticed any other symptoms yet.
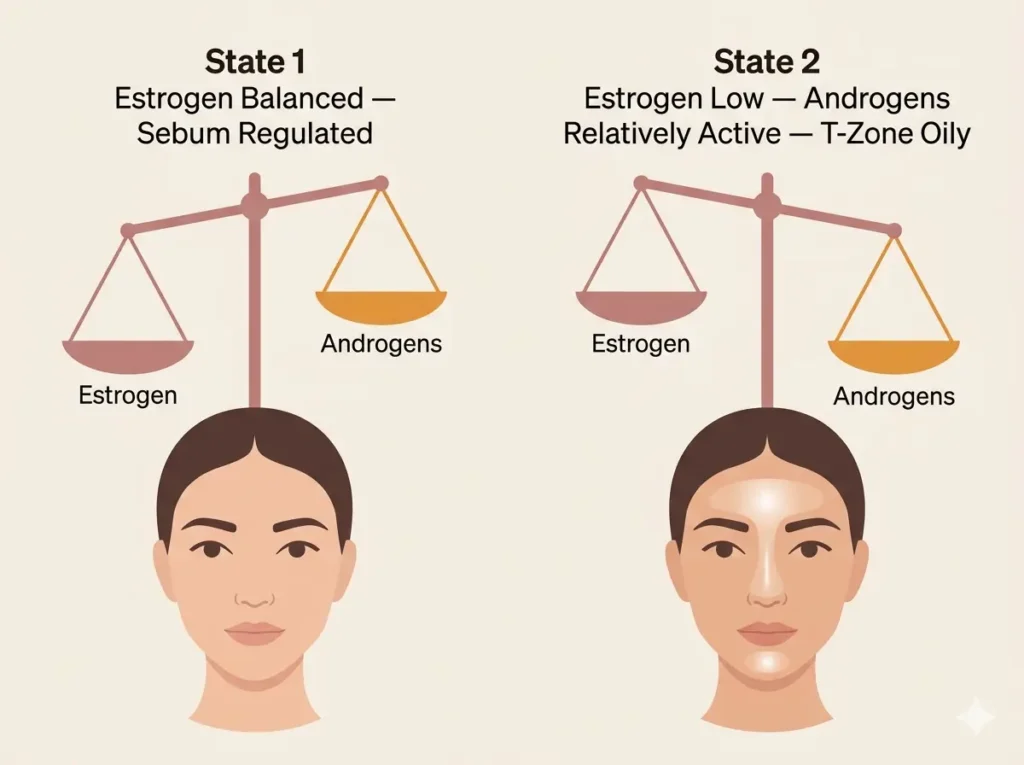
Yes, perimenopause can cause your skin to feel dry and oily at the same time. Falling estrogen weakens your skin barrier and reduces moisture. Meanwhile, androgen and cortisol fluctuations boost oil production in the T-zone — both happening on the same face simultaneously.
During perimenopause, estrogen levels drop unevenly. This reduces collagen and natural moisture retention in your skin. At the same time, androgens and cortisol can spike, triggering excess sebum in oilier zones like your forehead and nose — two separate hormonal processes producing opposite effects at once.
Perimenopause can begin as early as 35–38. Many women notice skin changes — including the dry-oily combination — before they notice anything else, like irregular periods or mood shifts.
Most women associate perimenopause with their mid-40s and missed periods. But skin changes frequently arrive years earlier — before cycles shift at all. That’s why so many women spend months troubleshooting products when the root cause is hormonal.
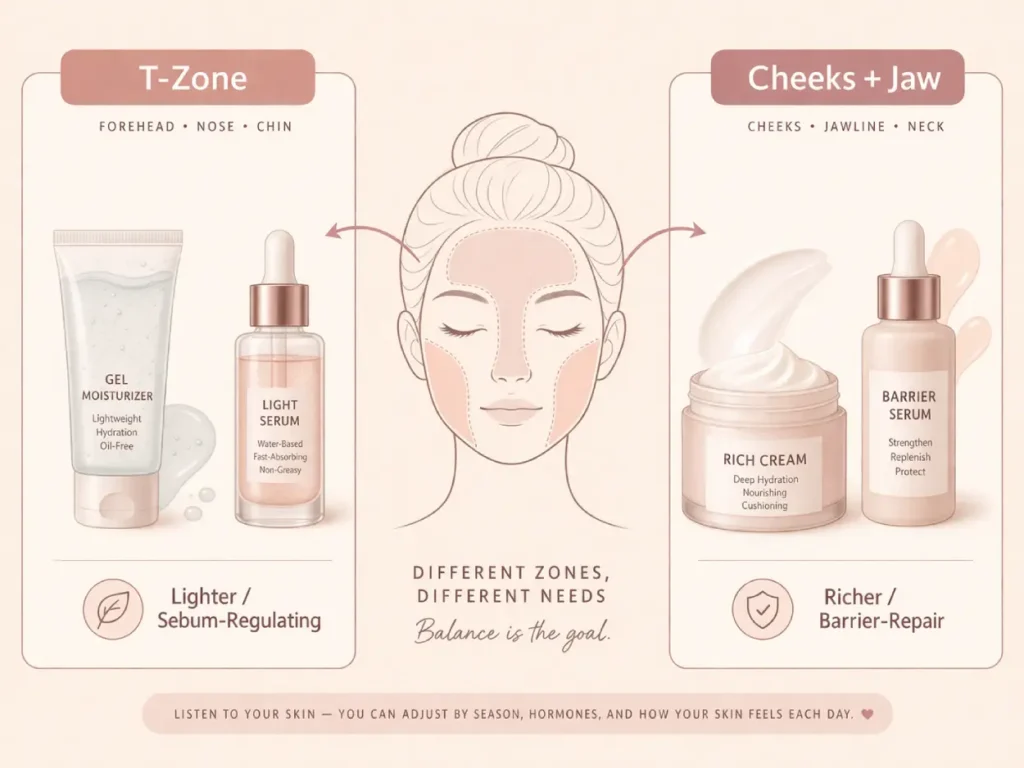
Zone-based skincare tends to work better than one product applied everywhere. Lighter, sebum-regulating products on the T-zone and barrier-repair ingredients on dry areas is the general approach. Ceramides, niacinamide, and peptides are the most consistently useful categories for this specific skin pattern.
Why Your Skin Feels Dry AND Oily at 38 — Perimenopause Explains It
You wash your face in the morning. By noon, your forehead is shiny. But your cheeks feel tight — almost like you forgot to moisturize. You did moisturize. Twice.
If this sounds familiar and you’re somewhere between 35 and 45, this probably isn’t a product problem. It’s a hormone problem. Specifically, it’s likely perimenopause — and it can start changing your skin years before your periods become irregular.
Here’s what’s actually happening.
1. What Is Perimenopause — And Why Does It Start Affecting Your Skin So Early
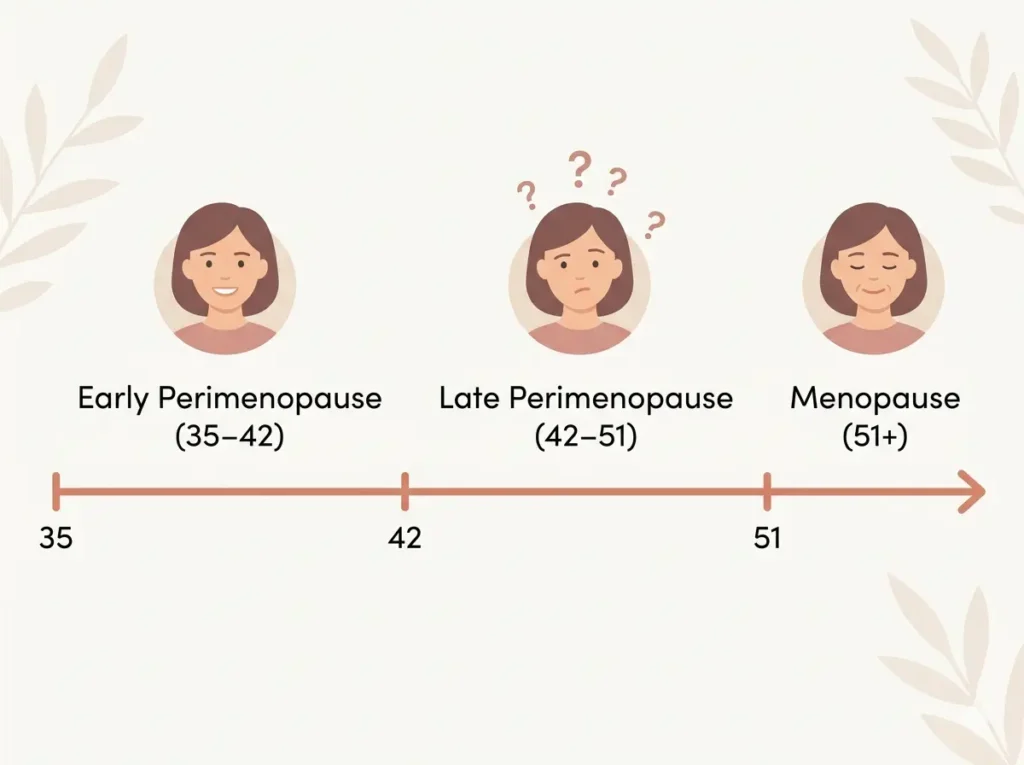
Perimenopause is the transition phase leading up to menopause. It’s not menopause itself — it’s the years before, when estrogen and progesterone levels start shifting unpredictably. For most women it begins between 35 and 45, though some notice changes earlier.
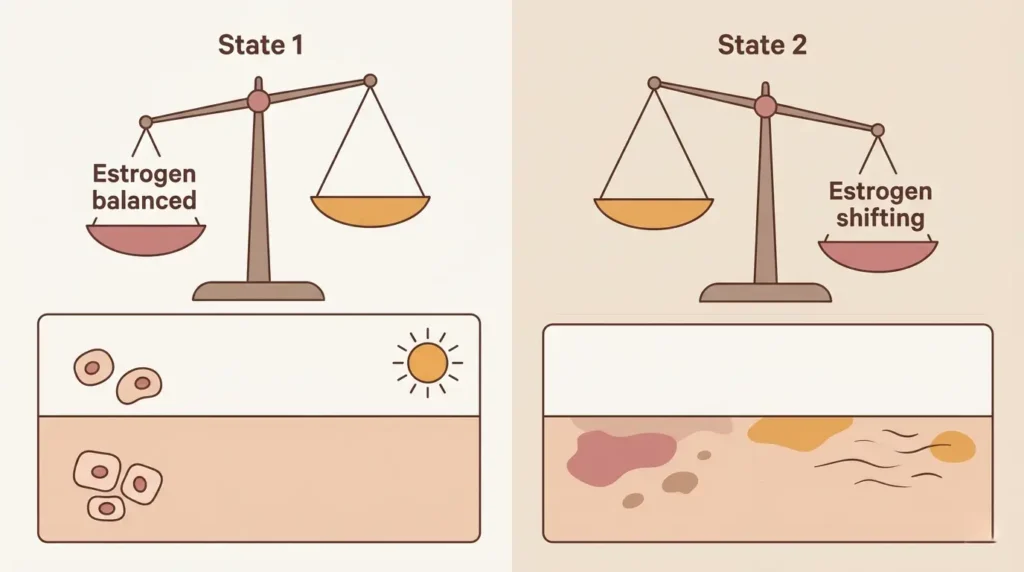
During this phase, hormones don’t just drop — they fluctuate. Some days levels are relatively normal. Other days they swing low. That inconsistency is part of what makes the symptoms so confusing.
Your skin is one of the first places these shifts show up because estrogen receptors live in skin tissue. When estrogen levels change, your skin responds fast.
What This Means: You don’t need irregular periods to be in perimenopause. Skin changes often arrive first — sometimes years before anything else feels different.
2. The Hormone Drop That Dries Your Skin Out
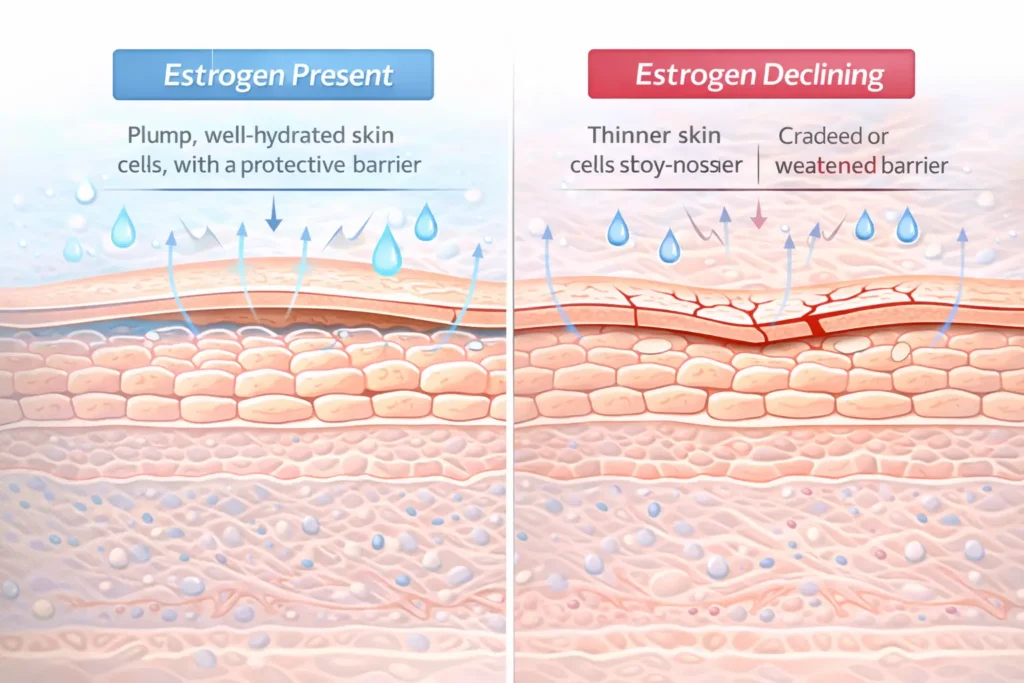
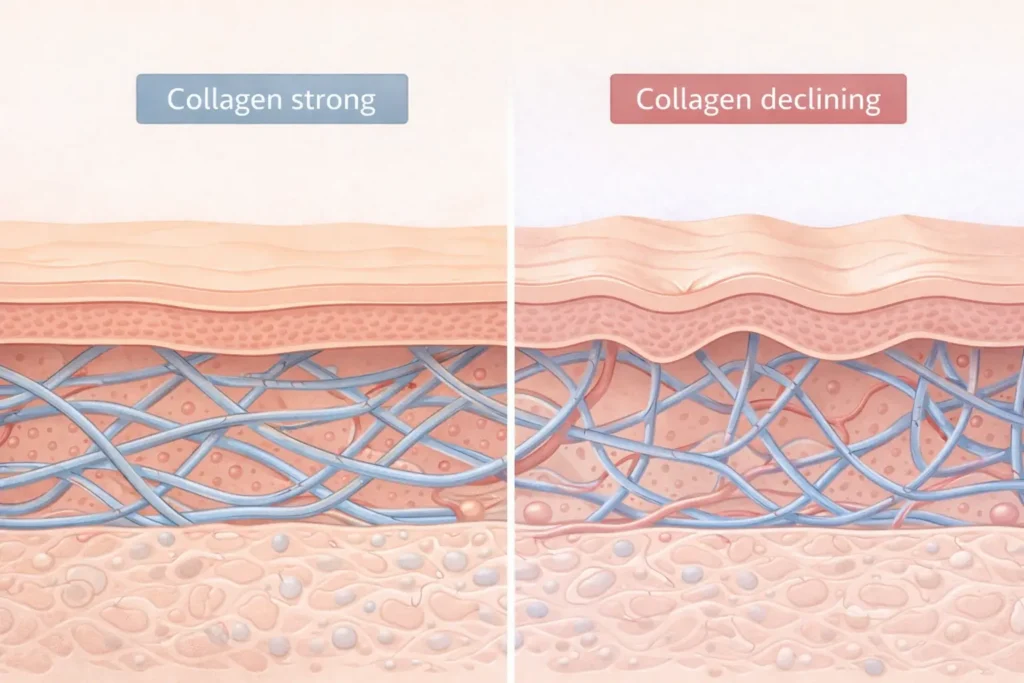
Estrogen plays a direct role in keeping your skin moist, thick, and elastic. It helps your skin produce hyaluronic acid — the substance that holds water in your skin cells. It also supports collagen production, which keeps your barrier strong.
When estrogen starts dropping during perimenopause, several things happen at once:
- Hyaluronic acid production slows — your skin holds less water
- Collagen starts declining — skin becomes thinner and less resilient
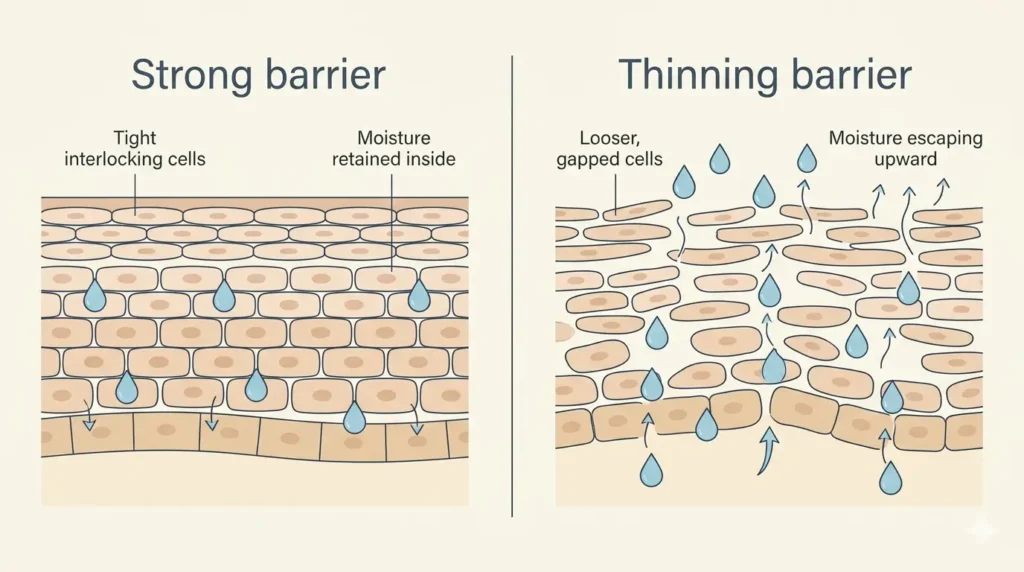
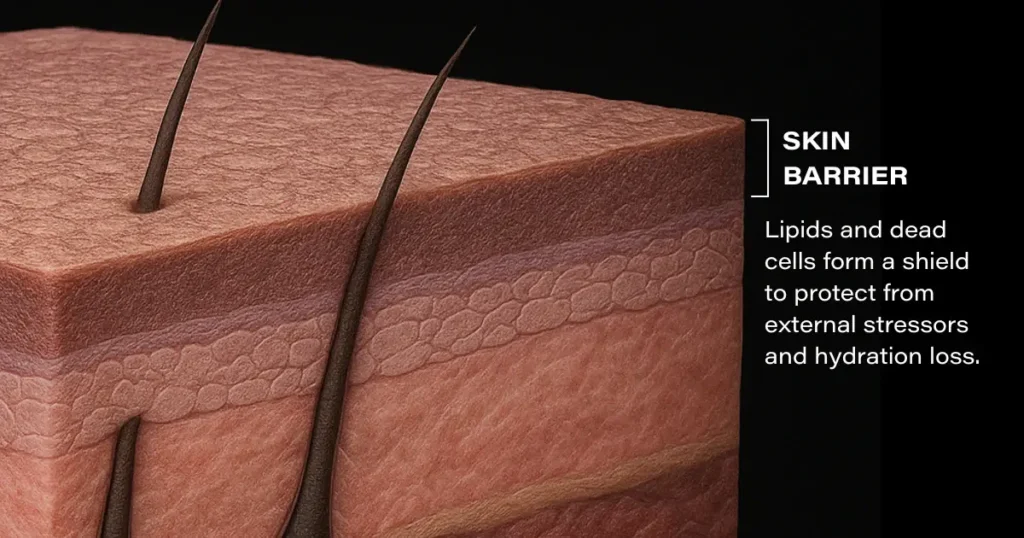
- The skin barrier weakens — moisture escapes faster than it should
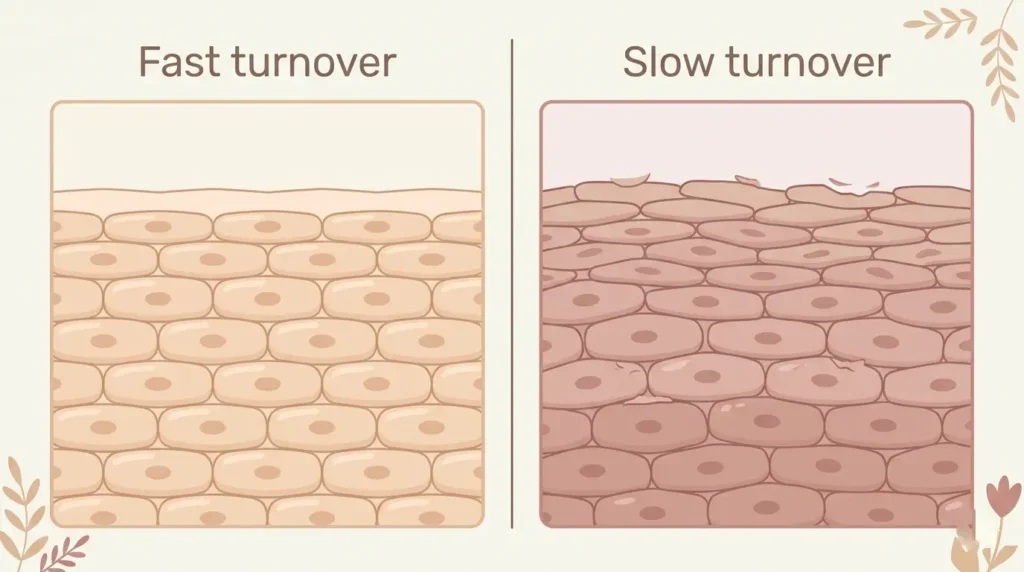
- Cell turnover slows — dead skin accumulates more easily
The result is skin that feels dry, tight, and sometimes almost papery — especially on your cheeks, jawline, and around your eyes.
Short Answer: Estrogen helps your skin hold moisture. When it drops during perimenopause, your skin barrier weakens and moisture escapes faster — causing dryness and tightness, especially on the cheeks and jaw.
3. Why Your T-Zone Is Still Oily (Even When the Rest of Your Face Feels Tight)
Here’s where it gets confusing. While estrogen is dropping, other hormones are fluctuating too — and some push in the opposite direction.
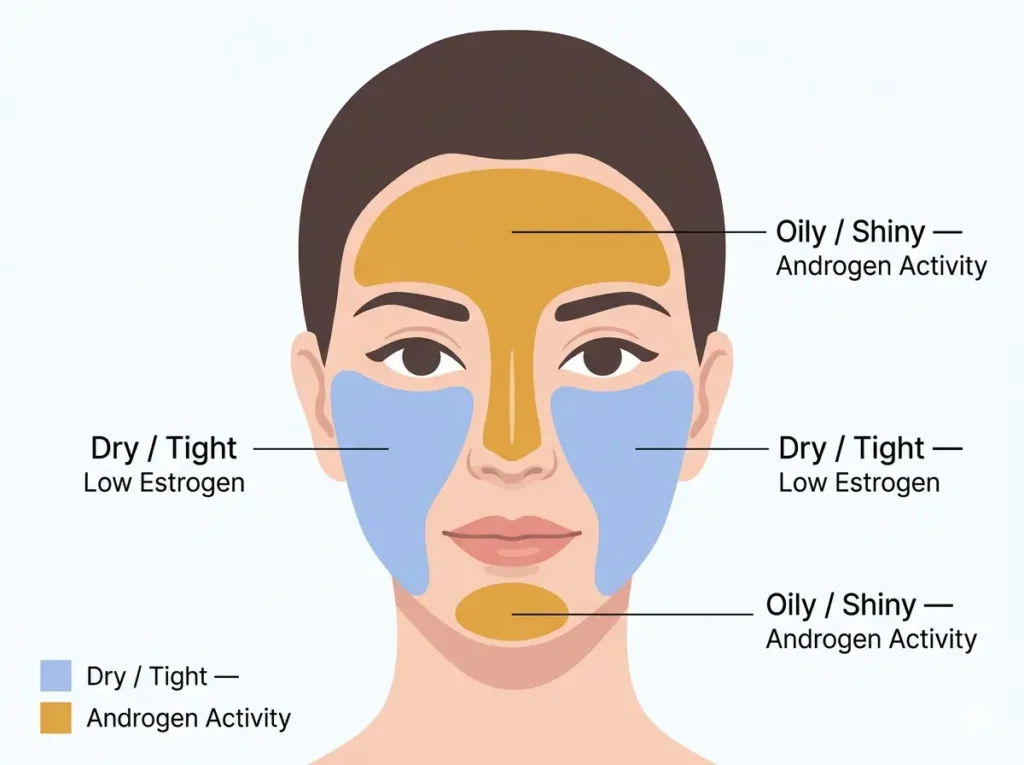
Androgens are hormones women also produce. During perimenopause, as estrogen drops, androgens become relatively more active by comparison. Androgens stimulate sebaceous glands — the glands that produce oil (sebum).
The T-zone has a higher concentration of sebaceous glands than the rest of your face. So when androgen activity increases, that’s where oil shows up most.
Cortisol — your stress hormone — can also rise during perimenopause due to disrupted sleep and hormonal instability. Cortisol is another known trigger for excess sebum production.
So you end up with:
- Dry, tight cheeks from low estrogen and a weakened barrier
- Oily forehead and nose from androgen and cortisol activity
Both happening on the same face. At the same time. That’s not a product failure — that’s two separate hormonal processes running simultaneously.
Short Answer: Androgens stimulate oil glands — especially in the T-zone. During perimenopause, estrogen drops but androgens stay relatively active, which is why your forehead and nose stay oily even when the rest of your face feels dry.
4. The Estrogen-Sebum Connection Most Skincare Brands Don’t Talk About
Most skincare marketing treats oily and dry skin as opposite problems needing opposite solutions. But perimenopause skin doesn’t work that way.
Estrogen helps regulate sebum production across the whole face. When estrogen is at healthy levels, oil production stays more balanced. When it drops, that regulation weakens — leaving oil glands more reactive to androgen signals, particularly in the T-zone.
This is why women who never had oily skin in their 20s can develop a greasy T-zone in their late 30s. It’s not a new skin type. It’s a shift in the hormonal system that was quietly keeping everything balanced.
What This Means: Combination skin appearing for the first time in your late 30s is often a hormonal signal — not a permanent change in your skin type. Treating it as a product problem without understanding the hormonal root usually leads straight to frustration.
5. Other Perimenopause Skin Symptoms That Show Up Around the Same Time
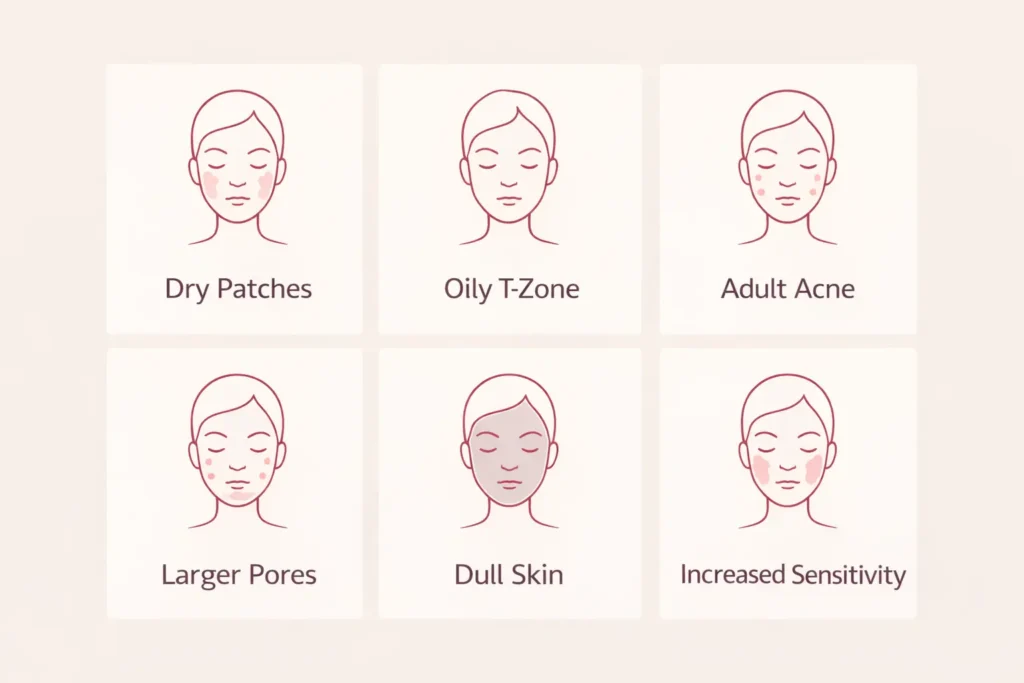
Dry-oily combination skin is rarely the only change. Around the same time, you might also notice:
- More visible pores — lower estrogen reduces skin thickness and elasticity, making pores appear larger
- Adult acne or breakouts — androgen activity and slowed cell turnover clog pores more easily
- Skin that reacts more easily — a weakened barrier makes skin sensitive to products it handled fine before
- Duller skin tone — slower cell turnover means dead skin stays on the surface longer
- Fine lines appearing faster — collagen decline accelerates during perimenopause
- Itchy or crawly skin — a lesser-known symptom linked to estrogen receptors in nerve endings
If you’re noticing two or more of these alongside the dry-oily confusion, perimenopause is a very likely explanation.
Short Answer: Common perimenopause skin changes include combination skin, adult acne, increased sensitivity, larger-looking pores, dullness, and faster-appearing fine lines — all driven by the same hormonal shifts.
6. What This Means for Your Current Skincare Routine
You don’t need to throw everything out. But understanding the hormonal root changes what to actually look for.
Support your barrier first. Look for ceramides, niacinamide, and peptides — ingredients that rebuild barrier function from the inside out — rather than just layering on more surface hydration.
Seal in your hyaluronic acid. On its own, HA can pull moisture out of skin in dry environments. Always layer it under a moisturizer that locks it in.
Add gentle exfoliation. Slower cell turnover means buildup happens faster now. A gentle chemical exfoliant once or twice a week clears the surface without stripping your barrier.
Try zone-based routines. Different products for different areas — lighter and mattifying on the T-zone, richer and barrier-focused on the cheeks and jaw — tend to outperform a single product applied everywhere during this skin transition.
What This Means: The goal isn’t to pick a skin type and treat the whole face the same way. It’s to support your barrier, regulate sebum gently, and meet each zone of your face where it actually is right now.
– FAQ –
Q1: Can perimenopause really start at 38?
Yes. Perimenopause typically begins between 35 and 45, with 38–42 being a common window. Hormonal fluctuations can begin much earlier than most women expect — skin changes, mood shifts, and sleep disruption are often among the first signs, even before periods become irregular.
Q2: Why is my skin both dry and oily at the same time?
Dropping estrogen dries out your skin barrier while androgen activity increases oil production in your T-zone — both happening simultaneously. The two processes are independent, which is why different parts of your face behave completely differently.
Q3: Does perimenopause cause combination skin?
Yes — many women develop combination skin during perimenopause even if they never had it before. Estrogen normally helps regulate sebum production across the face. When it drops, t
Q4: What does perimenopause skin feel like?
Inconsistent. Tight and dry on the cheeks and jawline, oily or shiny in the T-zone, more sensitive to products, and sometimes breaking out along the jaw or chin. Pores may look larger and skin tone duller than it used to be.
Q5: Can hormones cause oily skin in your late 30s?
Yes. Even if you had balanced or dry skin your whole life, androgen and cortisol fluctuations during perimenopause can introduce new oiliness — especially in the T-zone. This is one of the more surprising early perimenopause skin changes.
Q6: How do I know if my skin problems are from perimenopause?
The clearest indicator is unexplained change — you didn't switch products, diet, or environment, but your skin behaves differently. Combination skin appearing for the first time in your late 30s, alongside disrupted sleep, mood shifts, or irregular cycles, is a strong signal worth discussing with a doctor.
Q7: Does estrogen affect skin oil production?
Yes. Estrogen helps regulate sebum output across the face. When it drops during perimenopause, oil glands become more reactive to androgen signals — particularly in the T-zone — which is why oiliness and dryness can appear on the same face simultaneously.
Q8: What skincare ingredients help perimenopause combination skin?
Ceramides, niacinamide, peptides, and gentle chemical exfoliants are the most consistently recommended starting points. They support barrier repair, regulate sebum gently, and assist with cell turnover — without worsening either the dry or the oily zones.
Q9: Is it normal to get adult acne during perimenopause?
Yes. Adult acne — especially along the jawline and chin — is a common perimenopause symptom driven by androgen activity and increased sebum production. Slower cell turnover also means pores clog more easily than they used to.
Q10: Can perimenopause make your skin more sensitive?
Yes. Declining estrogen weakens the skin barrier, making skin more reactive to products, fragrances, and environmental triggers. Many women find that products they used for years suddenly cause irritation or redness during perimenopause.
Q11: At what age does perimenopause skin change start?
As early as 35–38 for many women, though the average onset is around 40–44. Skin changes are often among the earliest perimenopausal symptoms — sometimes appearing well before menstrual irregularities begin.
Q12: Should I see a doctor about perimenopause skin changes?
Yes — especially if the changes are significant or affecting your confidence. A dermatologist can address specific skin concerns, and a gynecologist or women's health specialist can assess whether hormonal support makes sense. Both perspectives working together tend to produce the best outcomes.