Quick Answers — Before You Read
What causes a widening part line in women?
A widening part line is caused by follicle miniaturization — a process where hair follicles progressively shrink and produce finer, shorter hairs with each growth cycle. In women over 35, declining estrogen is one of the most common triggers. The scalp becomes more visible at the part even without significant shedding because individual hairs are no longer thick enough to cover it the way they used to.
Is a wider part line a sign of low estrogen?
Yes, it can be. Estrogen keeps hair follicles in their active growth phase longer, supporting thicker and denser hair. When estrogen drops — especially during perimenopause or menopause — follicles shrink, hairs become finer with each cycle, and the part line gradually widens. This is one of the most common and most overlooked early signals of hormonal change in women between 35 and 58.
Is stress or hormones causing my thinning part?
Both can contribute, but they behave very differently. Stress causes telogen effluvium — sudden, temporary, widespread shedding that typically resolves within months. Hormonal thinning from estrogen decline is slow, concentrated at the part line and crown, and worsens over time without addressing the underlying shift. A part line that has been widening gradually for years is rarely explained by stress alone.
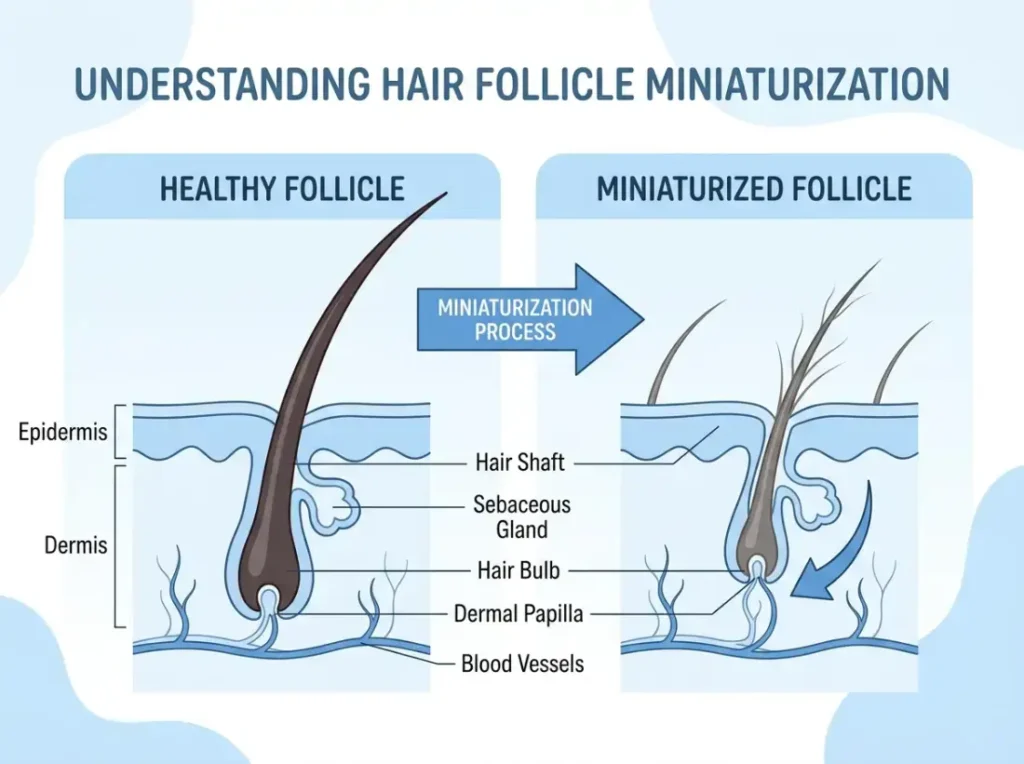
What is follicle miniaturization?
Follicle miniaturization is the process by which hair follicles progressively shrink, producing finer and shorter hairs with each growth cycle until they eventually become too small to produce visible hair. It is the core biological mechanism behind female pattern hair loss and is strongly driven by estrogen decline and rising DHT sensitivity. It is gradual, often goes unnoticed for years, and responds better to treatment the earlier it is caught.
When should I see a doctor about my widening part line?
See a doctor if thinning is rapid, patchy, or accompanied by symptoms like fatigue, irregular periods, weight changes, or skin changes. A dermatologist can assess the follicle pattern and rule out non-hormonal causes. A gynecologist or endocrinologist can evaluate your hormone levels. Even if thinning has been slow and gradual, a scheduled appointment is worthwhile — earlier intervention gives you more options.
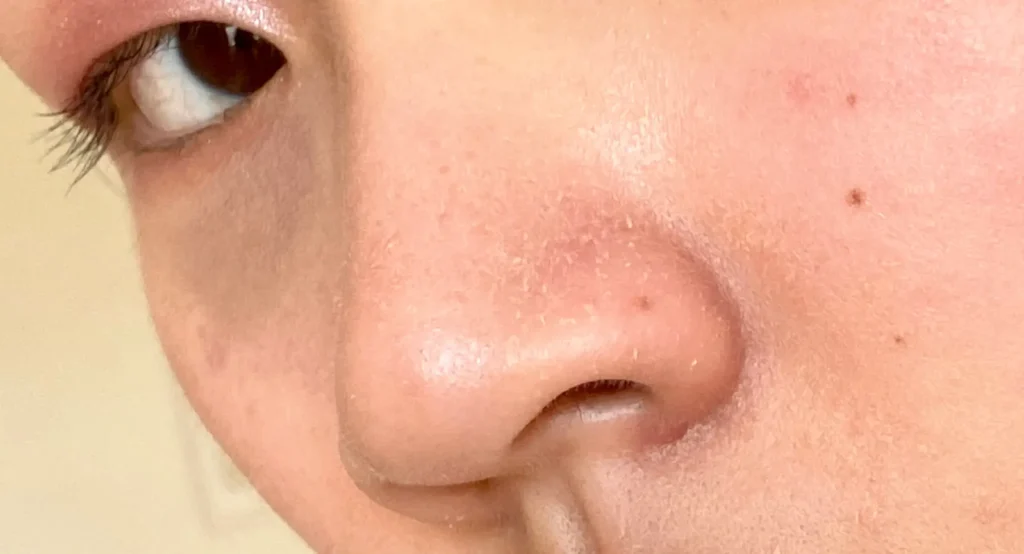
You noticed it in the bathroom mirror. Your part line — the strip of scalp that shows when you separate your hair — looked wider than it used to. You told yourself it was stress, your shampoo, or all the heat styling. And maybe some of that plays a role. But if the widening has been gradual, if it keeps happening no matter what you switch up, and if you’re somewhere between 35 and 58, there’s a good chance estrogen is at the center of this.
This article explains exactly what’s happening inside your follicles, why estrogen is the piece most people miss, and how to tell whether what you’re seeing is hormonal rather than just stress.
What a Widening Part Line Actually Means
Quick Take: A wider part doesn’t always mean you’re losing a lot of hair. It usually means your individual strands are getting finer — so your scalp shows through more easily than it used to.
Here’s something most people don’t realize: you don’t need to lose a significant amount of hair to have a visibly wider part line. What changes is the diameter and density of each individual strand.
When follicles are healthy and estrogen levels are strong, each strand grows thick enough that hairs naturally overlap and cover the scalp. As follicles shrink — a process called follicle miniaturization — the hairs they produce get progressively finer and shorter. They’re still there. They’re just not covering as well as they used to.
This is why a widening part can feel so sneaky. You’re not finding clumps in the shower drain. You’re not going bald. But something is visibly different, and it keeps getting worse. That gradual, quiet change is one of the hallmarks of female pattern hair loss — and estrogen decline is one of its biggest drivers.
The Estrogen-Hair Connection Most Women Don’t Know About
Quick Take: Estrogen is like a protective layer for your hair follicles. When it drops, follicles become more vulnerable to shrinkage — and your part line is usually one of the first places you see it.
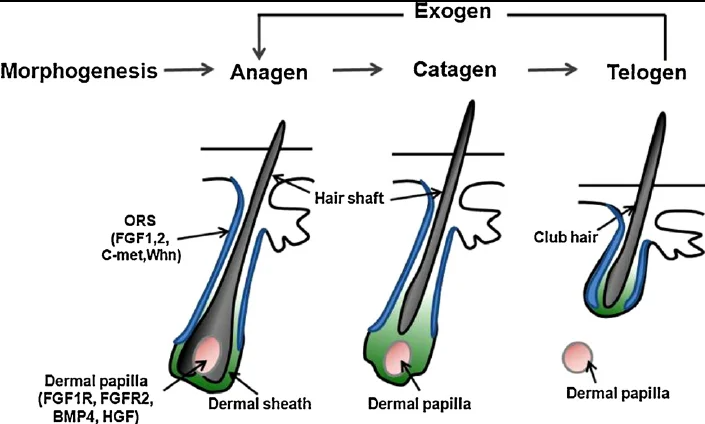
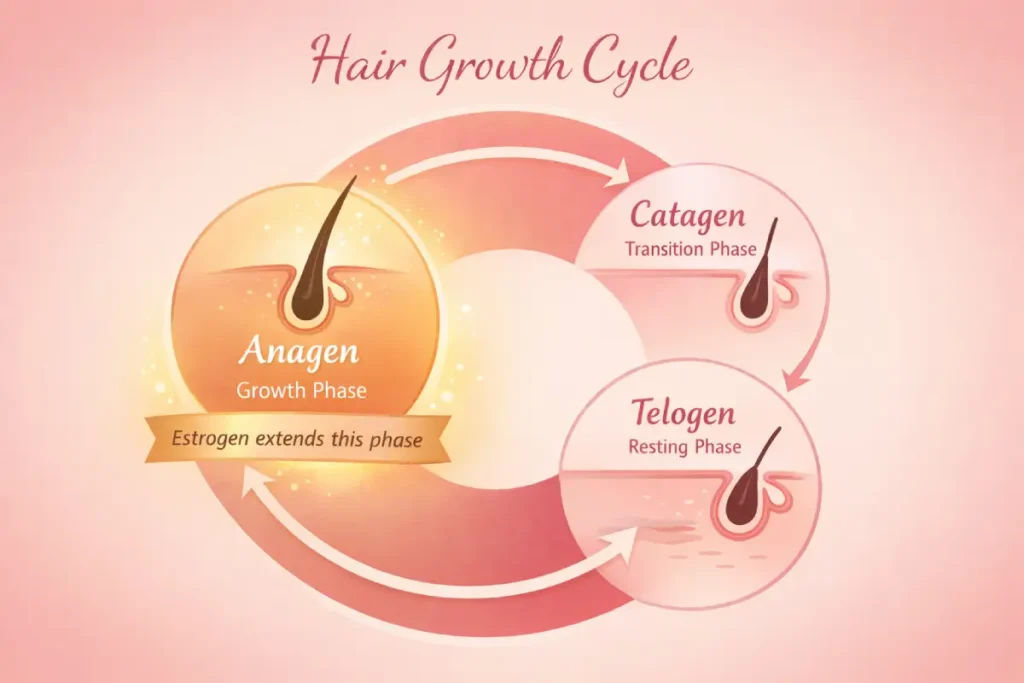
Your hair grows in a cycle. There’s a growth phase called anagen, a short transitional phase called catagen, and a resting phase called telogen where the hair eventually sheds before a new cycle begins.
Estrogen plays a direct role in keeping follicles in the anagen phase longer. Higher estrogen means longer growth cycles, which produces thicker, longer, and denser hair. This is why many women notice their hair looks its best during pregnancy, when estrogen is at its peak.
When estrogen starts declining, that protective effect weakens. Follicles spend less time in the growth phase and more time resting. Each new hair that grows comes in slightly finer than the last. Over months and years, the scalp becomes more visible — especially along the part line and at the crown, where this type of thinning tends to show up first.
There’s also a second layer to this. Lower estrogen shifts the hormonal balance toward androgens — male hormones like DHT that exist in small amounts in all women. DHT is well established as a follicle shrinker, and when estrogen isn’t there to help counterbalance it, its effects on the scalp become more pronounced. So it’s not just about losing estrogen. It’s about what happens to the whole hormonal ecosystem when estrogen steps back.
Why This Happens More After 35
Quick Take: Estrogen doesn’t wait for menopause to start declining. For many women, the shift begins in their mid-to-late 30s — and the hair part line is often one of the first places it shows.
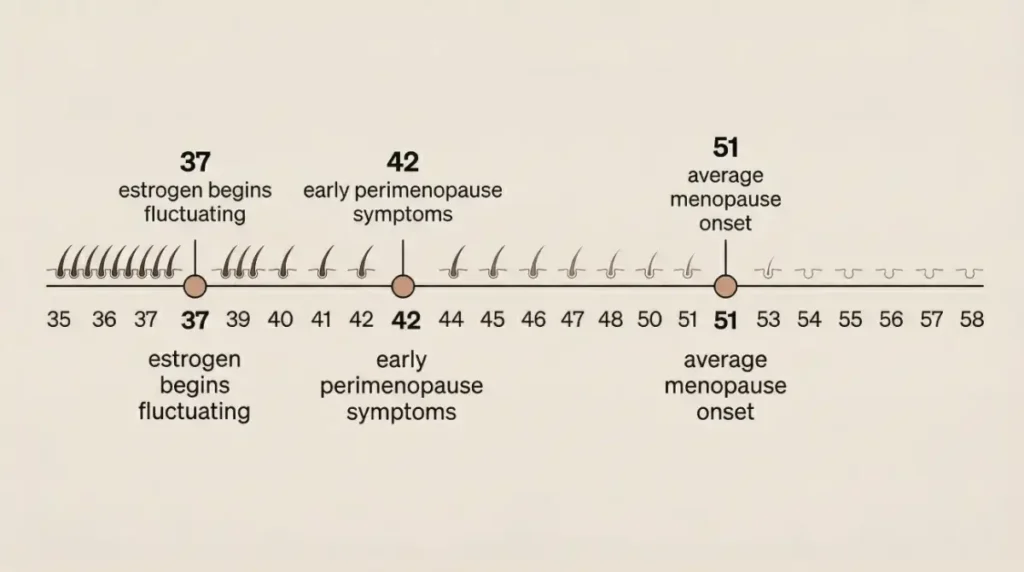
Most women associate hormonal changes with menopause, which typically happens in the early 50s. But the transition leading up to menopause — called perimenopause — can begin anywhere from 8 to 10 years earlier. That means some women start experiencing the effects of declining estrogen as early as their late 30s.
During perimenopause, estrogen doesn’t drop in a straight line. It fluctuates — sometimes surging, sometimes dipping — before eventually settling at lower levels permanently after menopause. These fluctuations are enough to disrupt the hair growth cycle repeatedly, even when periods are still regular and no other obvious symptoms have appeared yet.
This is why women in their late 30s and early 40s often feel blindsided. They’re not expecting hormonal hair changes. They think of menopause as years away. But their part line is widening, and nothing they try seems to help. The 35–58 window is when estrogen-related hair thinning becomes significantly more common — and significantly more under-discussed.
Stress vs. Hormones — How to Tell the Difference

Quick Take: Stress and hormonal thinning look similar on the surface but behave completely differently underneath. Knowing which one you’re dealing with changes how you respond.
Stress-related hair loss has a clinical name: telogen effluvium. It happens when a significant stressor — physical illness, emotional trauma, surgery, extreme dieting, or childbirth — pushes a large number of follicles into the resting phase simultaneously. About two to four months later, those hairs shed all at once.
The result is noticeable and often alarming, and it tends to spread across the whole scalp. But here’s the key thing: telogen effluvium is temporary. Once the stressor is removed and your body recovers, hair typically regrows within six to twelve months.
Hormonal thinning from estrogen decline works completely differently:
- It’s gradual, not sudden
- It’s concentrated at the part line and crown, not evenly spread
- It doesn’t resolve once the stressor passes — because there’s no single stressor causing it
- It worsens steadily over time without intervention
- It’s usually not accompanied by dramatic shedding — just slow, quiet miniaturization
If your part line has been widening gradually over one, two, or three years — without a major shedding event, without a clear stressor you can point to, and without any signs of improving — stress is probably not the primary explanation.
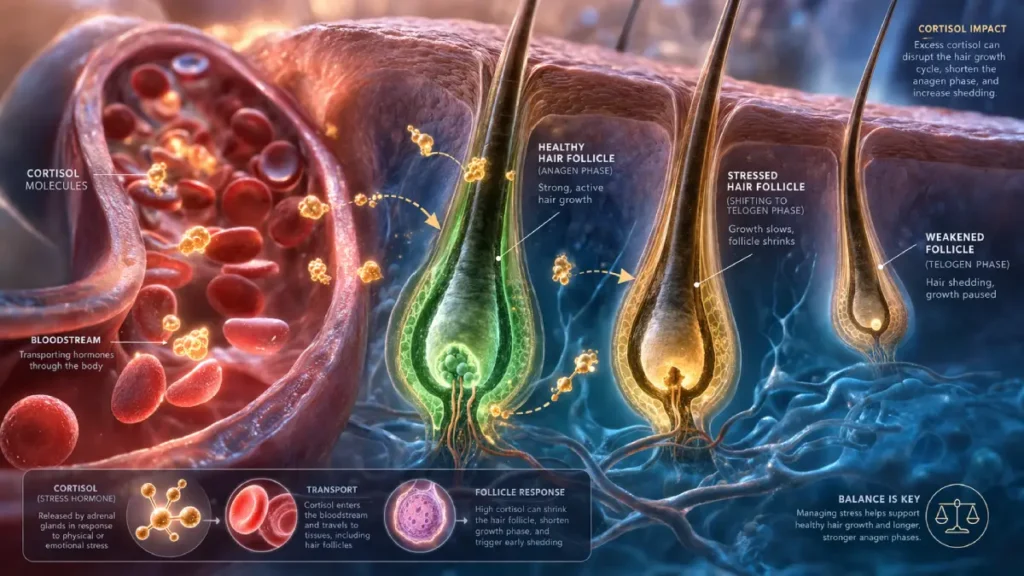
That said, chronic stress and hormonal imbalance often coexist. Elevated cortisol can worsen hormonal hair thinning by disrupting the body’s hormonal signaling. So stress isn’t irrelevant — it just probably isn’t the whole story.
Other Hormones That Affect Your Part Line
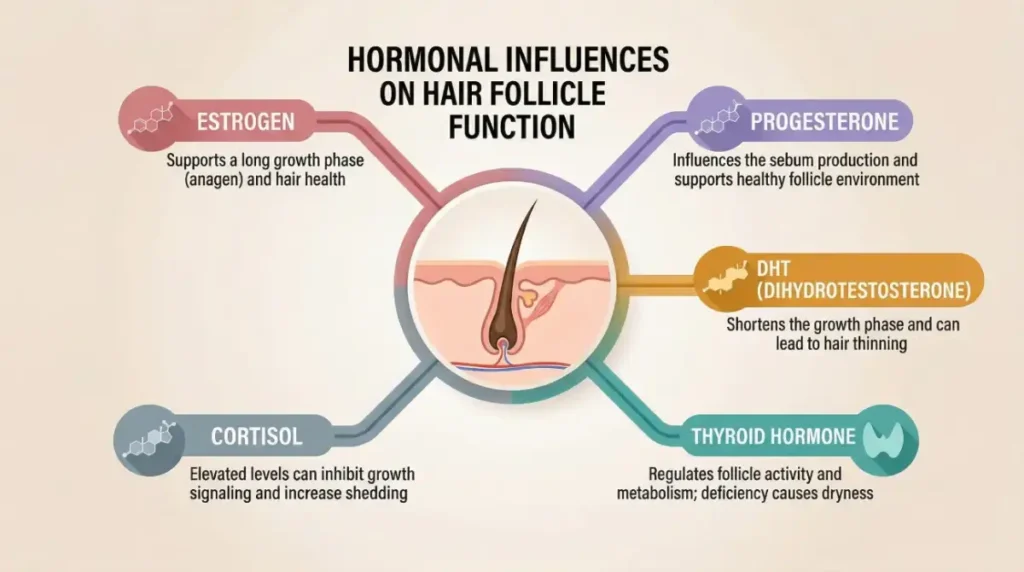
Quick Take: Estrogen gets most of the attention, but progesterone, DHT, thyroid hormones, and cortisol all affect your hair — and when estrogen declines, they all start exerting more influence at the same time.
Progesterone Progesterone works alongside estrogen and has its own hair-protective properties — including the ability to help block DHT at the follicle level. When progesterone declines alongside estrogen during perimenopause, the body loses two key hormonal counterweights simultaneously. That double decline creates a compounding effect: not only is estrogen’s growth-phase protection weakened, but DHT’s follicle-shrinking influence faces less resistance than it did before.
DHT (Dihydrotestosterone) With both estrogen and progesterone stepping back, DHT’s impact on follicles becomes significantly more pronounced. DHT is converted from testosterone and is the primary driver of androgenetic alopecia in both men and women. In women, rising DHT sensitivity tends to cause thinning concentrated at the part line and crown while the frontal hairline largely stays intact — a pattern sometimes called female androgenetic alopecia. It’s far more common in women over 35 than most people realize, and the hormonal context of perimenopause is often what tips it into visibility.
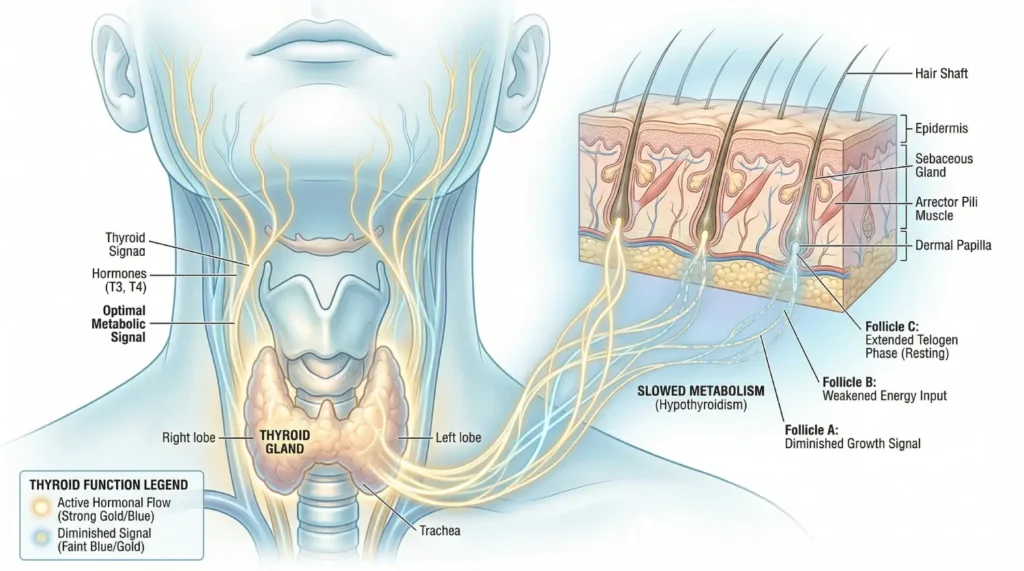
Thyroid Hormones The thyroid adds another layer to an already complex picture. Both an underactive thyroid (hypothyroidism) and an overactive thyroid (hyperthyroidism) can cause diffuse hair thinning, and thyroid imbalances are common in women over 35. They’re also frequently mistaken for stress or estrogen-related changes because the symptoms overlap significantly. If you’re experiencing fatigue, weight shifts, or sensitivity to temperature alongside your hair changes, thyroid function is worth evaluating as a separate variable.
Cortisol Chronic stress keeps cortisol elevated, which disrupts hormonal signaling across the board — including the signals that keep follicles in their growth phase. High cortisol doesn’t cause the dramatic shedding of acute stress, but it quietly amplifies existing hormonal thinning over time. Think of it as a background multiplier — it doesn’t start the fire, but it makes everything burn faster.
7 Signs Your Widening Part Line Is Hormonal
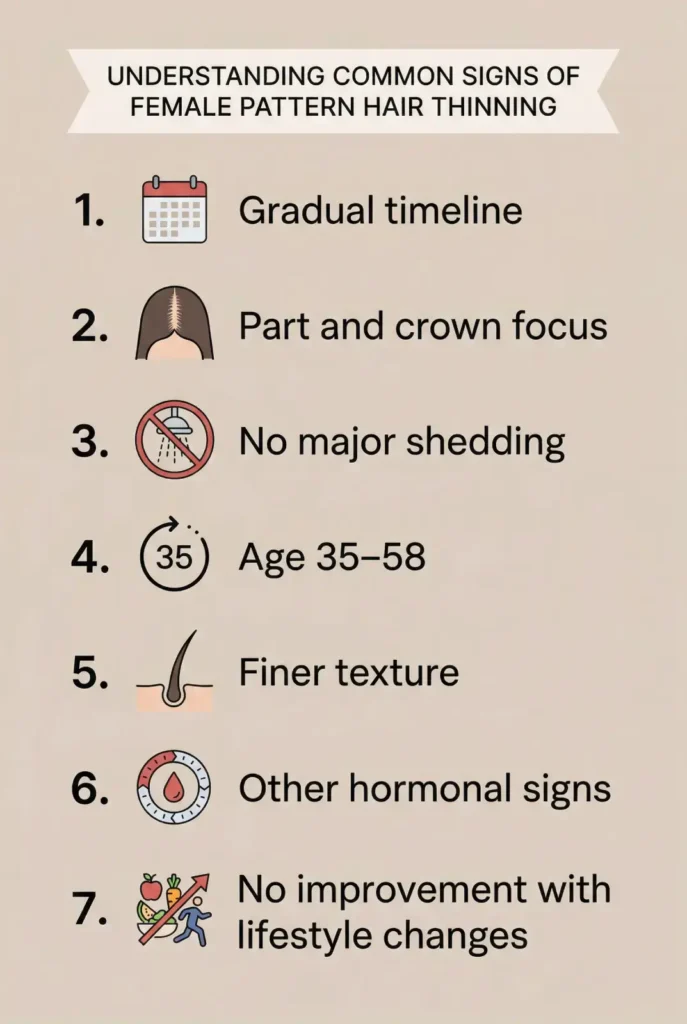
Taken together, these signs paint a clear picture of hormonal hair thinning — one that behaves differently from stress shedding, dietary deficiency, or any other common cause.
1. It’s been widening gradually over months or years Hormonal thinning is slow and progressive. If photos from two or three years ago show a noticeably fuller part, that timeline points directly to hormonal changes rather than a single stressor or temporary phase.
2. The thinning is concentrated at the part line and crown Female pattern hair loss from estrogen decline follows a predictable path — the part widens first, then the crown thins. The front hairline usually stays mostly intact. This is structurally different from stress shedding, which spreads more evenly.
3. You’re not seeing dramatic shedding If you’re not finding unusual amounts of hair in your brush or shower drain, but your part keeps widening, that’s follicle miniaturization — not acute shedding. The hairs are getting finer, not falling out in large numbers.
4. You’re between 35 and 58 This is the age window when estrogen fluctuation and decline have the most visible impact on hair. It doesn’t happen to every woman in this range, but age combined with the other signs in this list is a meaningful data point.
5. Your hair feels finer overall Beyond the part line, hormonal thinning often changes the full texture and feel of hair across the scalp. Ponytails feel noticeably thinner. Styles that used to hold don’t hold as well. Volume that used to be easy to create now requires more effort.
6. You’ve noticed other signs of hormonal change Irregular periods, sleep disruption, mood shifts, skin dryness, or brain fog alongside hair changes is a pattern worth paying attention to. Hair is rarely the only system estrogen affects when it starts shifting.
7. It’s not responding to lifestyle changes If you’ve improved sleep, cleaned up your diet, reduced stress, and your part line is still widening — that’s a strong signal the root cause isn’t lifestyle-based. Hormonal thinning requires addressing the actual hormonal driver, not just the surrounding conditions.
What You Can Do About It
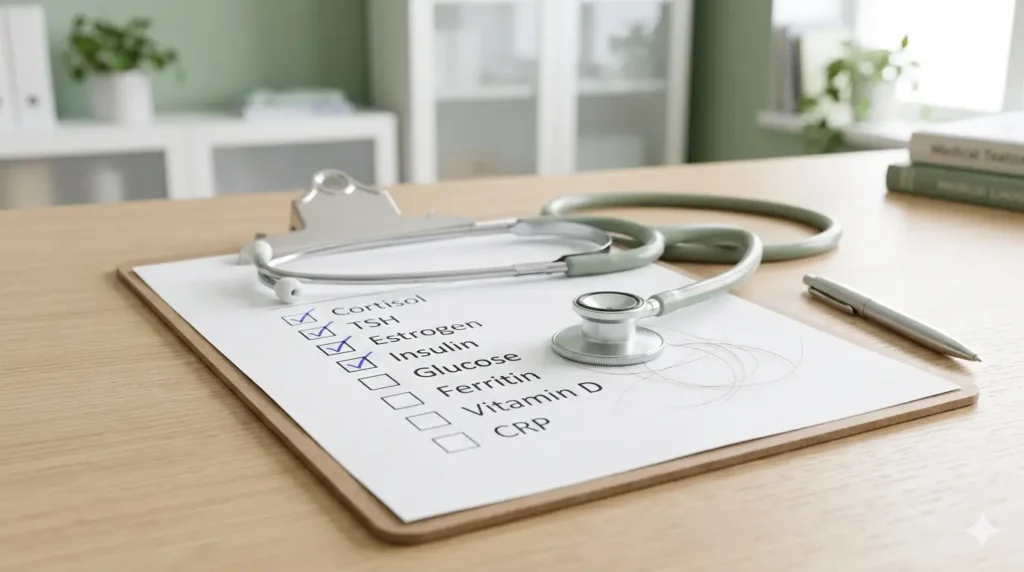
The most grounded starting points for hormonal hair thinning are a full hormone panel including ferritin, a consultation with a dermatologist who specializes in hair loss, and — where appropriate — clinically supported options like minoxidil, which is FDA-approved for female pattern hair loss. Early intervention consistently produces better outcomes than waiting.
Get your hormone levels checked A blood panel that includes estradiol, progesterone, total and free testosterone, DHEA-S, and a full thyroid panel gives you and your doctor a real picture of what’s happening. Don’t guess and don’t wait — the data changes the conversation.
Ask for ferritin specifically Low ferritin (stored iron) is one of the most commonly missed contributors to hair thinning in women. It frequently coexists with hormonal changes and makes everything worse. Many standard blood tests only check hemoglobin, which can look normal even when ferritin is critically depleted. Ask your doctor for ferritin by name — this one specific request has made a real difference for a lot of women.
Support your scalp environment Scalp inflammation can worsen follicle miniaturization over time. Gentle, sulfate-free cleansing, minimizing heat damage, and keeping the scalp healthy won’t reverse hormonal thinning on their own — but they create better conditions for any treatment to be effective.
Look into clinically supported topical options Minoxidil is FDA-approved for female pattern hair loss and has solid evidence behind it for slowing miniaturization and supporting regrowth. It’s available over the counter in 2% and 5% formulas for women. Talk to a dermatologist before starting — they can confirm whether it’s the right fit for your specific pattern.
See a dermatologist who knows hair A trichologist or dermatologist with experience in hair loss can perform a scalp analysis, review your hormone panel, and give you a clear personalized picture of what’s driving your thinning — including ruling out less common causes like alopecia areata or scarring conditions.
Don’t start with supplements alone The supplement market for hair growth is enormous and mostly unregulated. Some ingredients like saw palmetto and zinc have limited supporting evidence. Many have almost none. Supplements are not a substitute for identifying and addressing the actual root cause — start with the data, then layer in support.
When to See a Doctor ?

Some thinning patterns need professional evaluation sooner rather than later. These are the signals that mean don’t wait.
See a dermatologist or your primary care doctor if:
- Your part line is widening rapidly over weeks rather than months
- You’re noticing patchy hair loss rather than diffuse, gradual thinning
- You have bald spots or areas where the scalp looks shiny, smooth, or scarred
- Hair thinning is paired with significant fatigue, unexplained weight changes, or skin changes
- Your periods have become irregular or have stopped
- You’re losing hair in other areas — eyebrows, eyelashes, or body hair
- You’re under 35 and experiencing significant thinning with no obvious cause
Any of these patterns points to something beyond typical hormonal hair thinning and warrants a proper workup. The earlier you get an accurate diagnosis, the more options you have — and the better any treatment is likely to work.
FAQ
Q1. Can low estrogen really cause a wider part line?
Yes. Estrogen helps keep hair follicles in their active growth phase longer. When it declines, follicles shrink and produce finer hairs, making the scalp more visible at the part.
Q2. How do I know if my widening part is from stress or hormones?
Stress-related hair loss is usually sudden, temporary, and spread across the scalp. Hormonal thinning is gradual, concentrated at the part and crown, and doesn't reverse on its own.
Q3. At what age does estrogen-related hair thinning usually start?
It can begin as early as the mid-to-late 30s, during perimenopause — which can start up to a decade before full menopause.
Q4. Why is my hair thinning at the part but not falling out in clumps?
Because hormonal thinning works through miniaturization — hairs get finer and shorter with each cycle rather than falling out suddenly in large numbers.
Q5. Does estrogen make your hair thicker?
Yes. Estrogen prolongs the growth phase of the hair cycle and supports follicle health, resulting in thicker, denser hair.
Q6. Can perimenopause cause a widening part line even if my periods are regular?
Yes. Hormonal fluctuation during perimenopause can affect hair even when periods are still regular.
Q7. What hormones should I get tested if my part line is widening?
Ask for estradiol, progesterone, total and free testosterone, DHEA-S, a full thyroid panel (TSH, free T3, free T4), and ferritin.
Q8. Is a widening part line reversible?
It depends on the cause and how early you catch it. Addressing the underlying hormonal shift can slow or stop progression, and some regrowth is possible with appropriate treatment.
Q9. Does DHT cause hair loss in women the same way it does in men?
Yes, but typically less aggressively. DHT affects hair follicles in women too, especially when estrogen and progesterone decline and can no longer counterbalance its effects.
Q10. Should I see a dermatologist or gynecologist about my widening part line?
Ideally both. A dermatologist assesses your scalp and follicle health; a gynecologist or endocrinologist evaluates your hormone levels.
Q11. Can I slow my widening part line without hormone therapy?
Possibly, depending on severity and cause. Minoxidil, nutritional support, and scalp care are non-hormonal options with some evidence behind them.
Q12. How long does it take to notice improvement after addressing hormonal hair loss?
Most people need at least three to six months before seeing visible improvement, and full results can take up to a year.